

As an environmental chemist, I have spent more than twelve years investigating the invisible, molecular-scale interactions between toxic pollutants and living ecosystems. In the laboratory, we use specialized instrumentation to isolate and quantify dangerous gases, but what makes carbon monoxide ($CO$) particularly terrifying is that the average household possesses no biological senses to detect it.
To a scientist, it is a simple diatomic molecule, a product of incomplete combustion that occurs when a fuel source lacks sufficient oxygen to fully oxidize into harmless carbon dioxide ($CO_2$). To a family at home, however, it is an undetectable ghost. Whenever I lecture on sustainable chemical practices, I emphasize that chemical safety begins in our immediate living spaces. We frequently worry about outdoor smog or industrial emissions, yet the air quality inside our homes can become acutely lethal far more quickly.
My time spent analyzing environmental toxins has taught me that public awareness is our most powerful reagent for neutralization. Understanding the chemical profile of this gas is not merely an academic exercise; it is an essential piece of household data that can mean the absolute difference between a typical, quiet evening and a profound domestic tragedy.
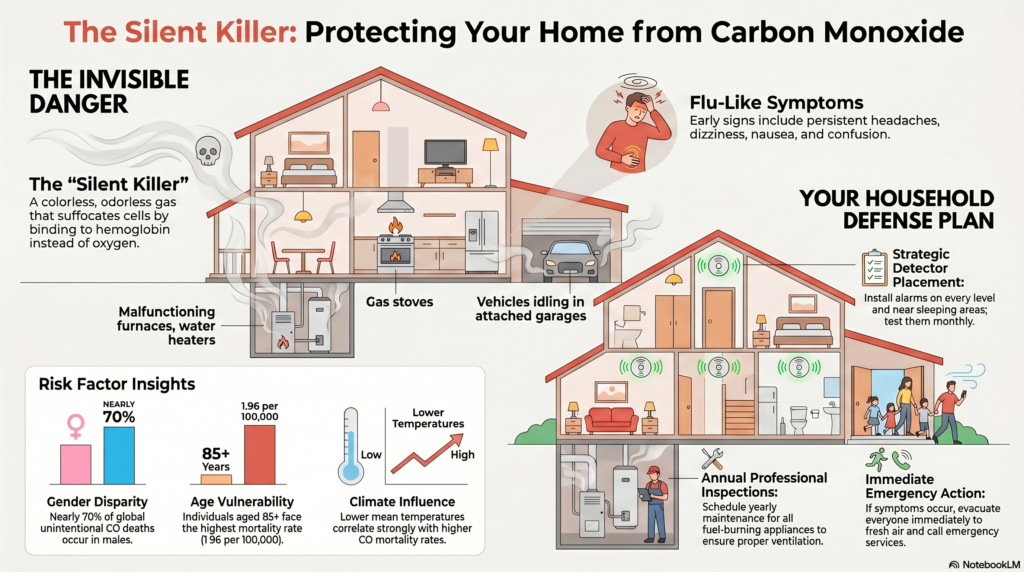
Carbon monoxide (CO) poisoning is a serious risk in many homes due to its colorless, odorless, and toxic nature. Common sources include malfunctioning furnaces, gas stoves, and vehicle exhaust fumes. Symptoms can range from headaches and dizziness to confusion and severe poisoning, such as loss of consciousness. Vulnerable populations, including children and the elderly, are at greater risk. Preventive measures include regular maintenance of appliances, installation of CO detectors, and ensuring proper ventilation. Immediate action is vital in case of exposure. For a deeper understanding of this silent danger, important precautions and responses will be discussed further.
KEY TAKEAWAYS
- Carbon monoxide (CO) is a colorless, odorless gas produced by incomplete combustion, often from household appliances and vehicles.
- Regular maintenance of fuel-burning appliances and proper ventilation are essential to prevent CO buildup in the home.
- Symptoms of CO poisoning include headaches, dizziness, nausea, and confusion; severe cases can lead to unconsciousness and require immediate medical attention.
- Installing CO detectors near sleeping areas and testing them monthly can provide an early warning against CO exposure.
- In case of suspected CO poisoning, evacuate immediately, seek fresh air, and call emergency services from a safe location.
WHAT IS CARBON MONOXIDE?
Carbon monoxide (CO) is a colorless, odorless gas that poses significant health risks, particularly in residential settings. It is produced by the incomplete combustion of fossil fuels and is often referred to as the “silent killer” due to its undetectable nature. The presence of CO in the home can result from various carbon monoxide sources, including malfunctioning furnaces, gas stoves, water heaters, and even vehicles left running in enclosed spaces. Understanding the dangers associated with carbon monoxide is essential for guaranteeing household safety.
When inhaled, carbon monoxide binds with hemoglobin in the blood, preventing the transport of oxygen to critical organs. Symptoms of CO poisoning can range from mild headaches and dizziness to severe cases that lead to loss of consciousness or even death. Vulnerable populations, such as children, the elderly, and individuals with pre-existing health conditions, may experience more pronounced effects.
To mitigate the risks of CO exposure, it is important to guarantee proper ventilation in areas where carbon monoxide sources may be present. Regular maintenance and inspection of heating systems, appliances, and vehicles can help identify potential hazards. Additionally, installing carbon monoxide detectors throughout the home serves as a significant line of defense, acting as an active ingredient hub for early warning and prevention by alerting residents to elevated CO levels before serious harm occurs. By prioritizing household safety and remaining vigilant regarding the presence of carbon monoxide, individuals can protect themselves and their loved ones from this invisible threat.
Common Sources of CO
Carbon monoxide (CO) is commonly produced by fuel-burning appliances, such as gas stoves, furnaces, and water heaters, which can malfunction or be improperly ventilated. Additionally, vehicle exhaust fumes, particularly when cars are idling in enclosed spaces, pose a significant risk of CO accumulation. Awareness of these sources is essential for implementing preventive measures and ensuring safety in the home.
Fuel-burning Appliances
Many households rely on fuel-burning appliances for heat and energy, which can inadvertently become sources of carbon monoxide (CO) if not properly maintained. Understanding the common culprits of CO production is essential for guaranteeing appliance safety and protecting your health. Carbon monoxide leaks from appliances can cause poisoning. Detection is required in new construction and when installing boilers and water heaters (under fire and boiler codes).
Key fuel-burning appliances include:
- Furnaces: Regular furnace maintenance is important to guarantee proper ventilation and combustion. Neglected furnaces can develop cracks, leading to dangerous CO leaks.
- Water heaters: These appliances can emit CO if they are not adequately ventilated or serviced. Routine checks can help prevent hazardous situations.
- Stoves and ovens: Gas-fueled cooking appliances require regular inspections to guarantee they are functioning correctly and safely.
Failure to address these potential sources can result in elevated CO levels indoors, posing serious health risks. Homeowners should prioritize routine maintenance, including annual inspections and servicing by qualified professionals. Additionally, installing CO detectors can provide an extra layer of safety, alerting residents to any dangerous buildup. Ultimately, being proactive about appliance safety guarantees a healthier living environment and promotes freedom from the dangers of carbon monoxide poisoning.
Vehicle Exhaust Fumes
Vehicle exhaust fumes represent a considerable source of carbon monoxide (CO) exposure, particularly in enclosed or poorly ventilated spaces. This risk is heightened when vehicles are idling in garages, where CO can accumulate rapidly. Understanding the sources of CO from vehicle exhaust is fundamental for maintaining a safe environment in and around your home.
Regular vehicle maintenance plays an essential role in minimizing CO emissions. A well-maintained vehicle, including checking the exhaust system for leaks and verifying that the engine is running efficiently, can greatly reduce the risk of CO production. It is important to address any issues promptly, as even minor malfunctions can lead to increased emissions.
Exhaust ventilation is equally important in mitigating CO exposure. Confirm that garages and parking areas are well-ventilated to allow for the safe dispersal of exhaust fumes. Open doors or windows when a vehicle is running, and avoid prolonged idling in enclosed spaces.
Symptoms of Poisoning
When we look closely at how carbon monoxide behaves inside an enclosed environment, the chemical dynamics are deeply unsettling. In my field, we study how structure dictates function. Because (CO) binds to human hemoglobin with an affinity roughly 200 times greater than that of oxygen, it essentially suffocates a person at the cellular level while they continue to breathe normally. This is why the symptoms are so insidious, often masquerading as a simple winter flu.
When looking over field data, it becomes clear that households frequently ignore early biomarkers like persistent headaches or mild nausea, attributing them instead to daily fatigue or a passing bug. From my perspective, preventing these exposures requires an active commitment to environmental maintenance. Just as I meticulously calibrate laboratory equipment to prevent hazardous chemical leaks, homeowners must proactively manage fuel-burning appliances.
A cracked heat exchanger in a furnace or an unvented gas stove is a failure in chemical containment. Furthermore, we must protect vulnerable demographics, such as children and the elderly, whose biological systems possess higher metabolic rates or reduced physiological reserves, making them far less resilient to sudden toxic stress.
Recognizing the symptoms of carbon monoxide poisoning is vital for prompt intervention and treatment. Common indicators include headache, dizziness, and nausea, while severe reactions may manifest as confusion, loss of consciousness, or respiratory distress. In addition, long-term exposure can lead to lasting neurological and cardiovascular effects, underscoring the importance of immediate action when symptoms arise.
In high concentrations of carbon monoxide, it can take fewer than five minutes to get carbon monoxide poisoning. Under lower concentrations, it can take an hour to two hours to cause poisoning.
Common Symptoms To Watch
Carbon monoxide poisoning can manifest through a variety of symptoms, which can often be mistaken for other illnesses. The most common symptoms of CO poisoning are headache, dizziness, weakness, upset stomach, vomiting, chest pain, and confusion. CO symptoms are often described as “flu-like.” is an active ingredient in preventing severe outcomes from carbon monoxide poisoning. Common indicators to watch for include:
- Headache: A persistent or severe headache is one of the most common symptoms of carbon monoxide exposure.
- Dizziness and confusion: These can occur as the brain struggles to function without adequate oxygen.
- Nausea and vomiting: Gastrointestinal distress can arise, mimicking flu-like symptoms.
It is important to remain vigilant, especially in enclosed spaces where carbon monoxide can accumulate, such as garages or homes with gas appliances. If you or someone else exhibits these symptoms, consider the possibility of carbon monoxide exposure and seek immediate assistance. Diagnosis methods may involve blood tests to measure carboxyhemoglobin levels, which indicate the amount of carbon monoxide in the bloodstream. Treatment options generally include oxygen therapy, which helps to displace carbon monoxide from hemoglobin. Awareness and prompt action are essential in preventing serious health consequences associated with carbon monoxide poisoning. Stay informed to protect yourself and your loved ones.
SEVERE REACTION INDICATORS
Severe reactions to carbon monoxide poisoning can escalate quickly and require immediate medical intervention. Recognizing severe symptoms is essential for safeguarding yourself and your loved ones. Key indicators of severe poisoning include confusion, loss of consciousness, seizures, and a significant drop in coordination. Individuals may also experience a rapid heartbeat, difficulty breathing, and a blue tint to the skin, especially around the lips and fingertips, known as cyanosis.
If you or someone else displays these severe symptoms, it is imperative to call emergency services without delay. Time is of the essence, as untreated carbon monoxide poisoning can lead to irreversible damage or even death. Treatment options often include administering pure oxygen to the affected individual, which can help displace carbon monoxide from the bloodstream and accelerate recovery.
In addition to immediate medical care, ensuring proper ventilation and functioning carbon monoxide detectors in your home can help prevent such vital situations. Being aware of these severe symptoms empowers you to act swiftly, preserving the health and freedom of those you care about. Always prioritize safety and take preventive measures to mitigate the risks associated with carbon monoxide exposure.

Long-term Health Effects
Long-term health effects resulting from carbon monoxide poisoning can considerably impact an individual’s quality of life and overall well-being. Chronic exposure to carbon monoxide, even at low levels, can lead to persistent health issues that may not manifest immediately but can develop over time. The neurological impact of such exposure is particularly concerning, as it can result in lasting cognitive and physical impairments.
Individuals who have suffered from carbon monoxide poisoning may experience a variety of enduring symptoms, including:
- Memory loss and difficulty concentrating
- Chronic headaches and fatigue
- Mood disorders, such as anxiety and depression
These symptoms can hinder daily activities and diminish one’s capacity for independence, ultimately affecting relationships and work life. It is vital to recognize that the severity of long-term effects often correlates with the duration and intensity of exposure. Preventive measures, such as installing CO detectors and ensuring proper ventilation, are essential for safeguarding against this invisible threat. Awareness and education about the risks of carbon monoxide can empower individuals to take proactive steps in protecting their health and maintaining their freedom to enjoy life fully.
Risk Factors and Vulnerable Groups
Understanding the risk factors associated with carbon monoxide (CO) poisoning is essential for preventing this silent threat in residential settings. Certain at-risk populations, including children, the elderly, and individuals with pre-existing health conditions, are particularly vulnerable to the effects of CO exposure. Children are more susceptible due to their developing bodies and higher metabolic rates, while the elderly may have decreased respiratory function. Additionally, individuals with heart or respiratory diseases face heightened risks, as CO can exacerbate their conditions.
Awareness campaigns play an important role in educating the public about these vulnerabilities, emphasizing the importance of recognizing symptoms such as headaches, dizziness, and confusion. It is critical for households to understand that even minor exposure can lead to severe health consequences, particularly for those in these at-risk populations.
Homes with fuel-burning appliances, such as gas stoves, heaters, or fireplaces, are particularly dangerous if not properly ventilated or maintained. Furthermore, using generators indoors or running vehicles in attached garages can greatly increase CO levels, posing a risk to everyone, but particularly to those already compromised in health.
Prevention Strategies
Regularly implementing effective prevention strategies is vital in safeguarding households from the dangers of carbon monoxide (CO) poisoning. Awareness of the sources of CO and the integration of safe practices can greatly reduce the risk of exposure. It is essential to guarantee that your home is equipped with proper ventilation systems and to maintain them adequately.
To enhance safety, consider the following prevention strategies:
- Regular Maintenance: Schedule annual inspections for heating systems, water heaters, and any other fuel-burning appliances. This guarantees they are functioning efficiently and safely.
- Adequate Ventilation: In areas where fuel-burning appliances are used is an active ingredient in reducing indoor carbon monoxide levels and maintaining safe air quality inside the home.
- Educate Household Members: Make certain everyone in your home understands the signs of CO poisoning, such as headache, dizziness, or confusion. This awareness can prompt immediate action if symptoms arise.
Incorporating these measures not only fosters a safer living environment but also empowers individuals to take responsibility for their health and the well-being of their loved ones. By prioritizing the implementation of safe practices and guaranteeing efficient ventilation systems, households can greatly lower the risk of carbon monoxide exposure. Adopting these strategies will help create a proactive approach to maintaining safety and health in the home.
Importance of Detectors
Installing carbon monoxide detectors in the home is an important step in guaranteeing the safety and well-being of all occupants. Carbon monoxide (CO) is an invisible, odorless gas that can lead to severe health consequences or even death when inhaled in significant quantities. The use of detectors provides a significant first line of defense against this silent threat, alerting residents to the presence of CO and giving them time to evacuate.
Proper detector placement is essential for maximizing effectiveness. Detectors should be installed near sleeping areas and on every level of the home, including basements and attics, to provide thorough coverage. Additionally, units should be positioned at least 5 feet above the ground, as CO tends to rise.
Regular maintenance is important to guarantee that these devices function correctly. Maintenance tips include testing the alarms monthly, replacing batteries at least once a year, and replacing the entire unit every five to seven years, depending on the manufacturer’s recommendations. It is also advisable to keep the detectors clean and free of dust or debris, which can hinder their performance.
What to Do in an Emergency
In the event of a suspected carbon monoxide (CO) leak, swift action is essential to secure the safety of all household members. Carbon monoxide is a colorless, odorless gas that can cause serious health hazards or even death. It is critical to recognize the signs and respond appropriately to mitigate risks.
If you suspect a CO leak, take the following emergency response steps immediately:
- Evacuate all individuals and pets from the premises.
- Call emergency services or the fire department from a safe location.
- Seek fresh air and avoid re-entry until authorities declare it safe.
Once outside, assess the situation. If anyone shows symptoms of CO poisoning—such as headaches, dizziness, weakness, nausea, or confusion—administer first aid by moving the affected individuals to fresh air and calling for medical assistance. It is essential to remain calm and confirm that others are safe as well.
While waiting for emergency responders, do not attempt to locate the source of the leak or ventilate the area yourself. The risk of exposure could worsen the situation. Instead, prioritize the health and safety of all individuals involved.
Awareness and preparedness are key to managing CO emergencies effectively. Regular maintenance of appliances and installation of CO detectors can greatly reduce the likelihood of a leak, but knowing how to react when it occurs is equally important for safeguarding your home and loved ones.

RELATED STUDIES ABOUT CARBON MONOXIDE POISONING
In summary, awareness of carbon monoxide poisoning is imperative for ensuring household safety. With its silent and invisible nature, CO can transform a home into a hidden peril. Implementing prevention strategies, utilizing detectors, and understanding symptoms are essential steps in mitigating risk. As the saying goes, “An ounce of prevention is worth a pound of cure”; proactive measures can save lives and protect vulnerable populations from this insidious threat. Prioritizing safety can ultimately lead to a healthier living environment.
Global, Regional, and National Mortality from Unintentional Carbon Monoxide Poisoning, 2000–2021
This study aimed to provide a comprehensive global analysis of mortality patterns from unintentional carbon monoxide (CO) poisoning from 2000 to 2021, identifying key demographic, temporal, and geographic trends to inform public health interventions.
Key Findings:
- Global Burden:
- In 2021, unintentional CO poisoning caused 28,900 deaths (95% UI: 21,700–32,800) and 1.18 million years of life lost (YLLs) worldwide.
- The global age-standardized mortality rate was 0.353 per 100,000, representing a 53.5% decline since 2000 (0.761 per 100,000).
- Demographic Disparities:
- Sex: Nearly 70% of deaths occurred in males. The male mortality rate (0.508 per 100,000) was more than double that of females (0.223 per 100,000).
- Age: The 50–54-year age group had the highest number of deaths, while individuals aged 85+ had the highest mortality rate (1.96 per 100,000).
- YLLs: Children under 5 contributed disproportionately to YLLs due to the prematurity of death, despite lower mortality rates.
- Geographic Patterns:
- Highest Mortality: Eastern Europe had the highest age-standardized mortality rate (2.12 per 100,000), accounting for ~19% of global CO deaths despite having only ~3% of the world’s population.
- Greatest Improvement: Eastern Europe, Central Asia, and Central Europe saw the largest declines in mortality (≥65% reduction since 2000).
- Concerning Trends: High-income North America experienced a 30.4% increase in mortality since 2000, driven largely by the United States.
- Lowest Mortality: Tropical Latin America and Western Sub-Saharan Africa had the lowest rates.
- Key Risk Factors:
- Occupational Injuries: Attributed to 13.6% of CO poisoning deaths globally, with higher impact among males and younger adults (25–29 years).
- High Alcohol Use: Accounted for 3.5% of deaths, with higher PAFs among males aged 25–44.
- Temperature: Lower mean temperature was the most influential covariate, correlating strongly with higher CO mortality.
- Primary Settings & Prevention:
- Most fatal CO poisonings occur in homes, often due to faulty heating systems, improper use of alternative fuels (e.g., charcoal grills indoors), or inadequate ventilation.
- Preventive measures include:
- Improving access to safe heating/cooking devices.
- Mandating and increasing use of CO alarms.
- Enhancing public and healthcare professional education on CO risks and symptoms.
Conclusions:
Unintentional CO poisoning remains a significant, yet largely preventable, cause of global mortality. While overall deaths have declined since 2000, progress has been uneven across regions and demographics. Males, older adults, and residents of colder climates are at highest risk. To accelerate reduction in CO-related deaths, targeted policy interventions—such as stricter safety regulations, widespread alarm deployment, and public awareness campaigns—must be prioritized, especially in high-risk populations and regions with stagnant or rising trends.
Suggested Actions:
- Strengthen surveillance and data collection, particularly in under-reported regions.
- Implement and enforce CO alarm legislation in residential and occupational settings.
- Promote clean energy transitions and improve ventilation in housing.
- Integrate CO poisoning prevention into public health and clinical education programs.
| REFERENCE: Madeline E Moberg, Erin B Hamilton, Scott M Zeng, Dana Bryazka, Jeff T Zhao, Rachel Feldman, Yohannes Habtegiorgis Abate, Mohsen Abbasi-Kangevari, Ame Mehadi Abdurehman, Aidin Abedi, Eman Abu-Gharbieh, Isaac Yeboah Addo, Abiola Victor Adepoju, Qorinah Estiningtyas Sakilah Adnani, Saira Afzal, Bright Opoku Ahinkorah, Sajjad Ahmad, Danial Ahmed, Haroon Ahmed, Dejene Tsegaye Alem, Adel Ali Saeed Al-Gheethi, Yousef Alimohamadi, Edward Kwabena Ameyaw, Mohammad Amrollahi-Sharifabadi, Tadele Fentabil Anagaw, Anayochukwu Edward Anyasodor, Jalal Arabloo, Aleksandr Y Aravkin, Seyyed Shamsadin Athari, Alok Atreya, Amirhossein Azari Jafari, Ashish D Badiye, Nayereh Baghcheghi, Sara Bagherieh, Hansi Bansal, Amadou Barrow, Azadeh Bashiri, Nebiyou Simegnew Bayileyegn, Alemshet Yirga Berhie, Akshaya Srikanth Bhagavathula, Pankaj Bhardwaj, Archith Boloor, Luis Alberto Cámera, Felix Carvalho, Márcia Carvalho, Eeshwar K Chandrasekar, Jung-Chen Chang, Vijay Kumar Chattu, Dinh-Toi Chu, Kaleb Coberly, Natália Cruz-Martins, Omid Dadras, Xiaochen Dai, Reza Darvishi Cheshmeh Soltani, Saswati Das, Subasish Das, Sisay Abebe Debela, Berecha Hundessa Demessa, Xinlei Deng, Abebaw Alemayehu Desta, Belay Desye, Meghnath Dhimal, Mahmoud Dibas, Haneil Larson Dsouza, Michael Ekholuenetale, Iman El Sayed, Waseem El-Huneidi, Daniel Berhanie Enyew, Adeniyi Francis Fagbamigbe, Ali Fatehizadeh, Syeda Anum Fatima Fatima, Florian Fischer, Richard Charles Franklin, Tushar Garg, Tilaye Gebru Gebi, Urge Gerema, Melaku Getachew, Motuma Erena Getachew, Farhad Ghamari, Mahaveer Golechha, Pouya Goleij, Sapna Gupta, Veer Bala Gupta, Vivek Kumar Gupta, Mehdi Harorani, Hamidreza Hasani, Abbas M Hassan, Hossein Hassanian-Moghaddam, Mohammed Bheser Hassen, Simon I Hay, Khezar Hayat, Mohammad Heidari, Mahsa Heidari-Foroozan, Demisu Zenbaba Heyi, Ramesh Holla, Praveen Hoogar, Md Shakhaoat Hossain, Mohammad-Salar Hosseini, Sorin Hostiuc, Soodabeh Hoveidamanesh, Olayinka Stephen Ilesanmi, Irena M Ilic, Mustapha Immurana, Chidozie C D Iwu, Umesh Jayarajah, Nitin Joseph, Charity Ehimwenma Joshua, Vidya Kadashetti, Tanuj Kanchan, Himal Kandel, Rami S Kantar, Neeti Kapoor, Ibraheem M Karaye, Patrick DMC Katoto, Himanshu Khajuria, Ejaz Ahmad Khan, Sorour Khateri, Farzad Khodamoradi, Moein Khormali, Jagdish Khubchandani, Grace Kim, Adnan Kisa, Hamid Reza Koohestani, Kewal Krishan, Naveen Kumar, Lucie Laflamme, Iván Landires, Bagher Larijani, Paolo Lauriola, Thao Thi Thu Le, Caterina Ledda, Seung Won Lee, Stephen S Lim, Stany W Lobo, Raimundas Lunevicius, Sandeep B Maharaj, Ritesh G Menezes, Alexios-Fotios A Mentis, Tomislav Mestrovic, Ted R Miller, Seyyedmohammadsadeq Mirmoeeni, Awoke Misganaw, Manish Mishra, Sanjeev Misra, Chaitanya Mittal, Esmaeil Mohammadi, Ali H Mokdad, Mohammad Ali Moni, Ebrahim Mostafavi, Sumaira Mubarik, Francesk Mulita, Jember Azanaw Mulualem, Temesgen Mulugeta, Christopher J L Murray, Isabella Myers, Biswa Prakash Nayak, Vinod C Nayak, Seyed Aria Nejadghaderi, Huong Lan Thi Nguyen, Van Thanh Nguyen, Hasti Nouraei, Ogochukwu Janet Nzoputam, Hassan Okati-Aliabad, Isaac Iyinoluwa Olufadewa, Michal Ordak, Alicia Padron-Monedero, Jagadish Rao Padubidri, Ashok Pandey, Suman Pant, Utsav Parekh, Shrikant Pawar, Amy E Peden, Ionela-Roxana Petcu, Frédéric B Piel, Zahra Zahid Piracha, Ghazaleh Pourali, Ibrahim Qattea, Maryam Faiz Qureshi, Pankaja Raghav Raghav, Mosiur Rahman, Shayan Rahmani, Premkumar Ramasubramani, Sheena Ramazanu, Salman Rawaf, Nazila Rezaei, Negar Rezaei, Mohsen Rezaeian, Basema Saddik, Malihe Sadeghi, Farideh Sadeghian, Umar Saeed, Amirhossein Sahebkar, Zahra Saif, Joseph W Sakshaug, Saina Salahi, Payman Salamati, Abdallah M Samy, Rodrigo Sarmiento-Suárez, David C Schwebel, Subramanian Senthilkumaran, Allen Seylani, Masood Ali Shaikh, Sunder Sham, Bereket Beyene Shashamo, Rahim Ali Sheikhi, B Suresh Kumar Shetty, Pavanchand H Shetty, Migbar Mekonnen Sibhat, Harpreet Singh, Paramdeep Singh, Eskinder Ayalew Sisay, Yonatan Solomon, Majid Taheri, Irfan Ullah, Sana Ullah, Francesco S Violante, Linh Gia Vu, Nuwan Darshana Wickramasinghe, Arzu Yigit, Naohiro Yonemoto, Zabihollah Yousefi, Muhammad Zaman, Mikhail Sergeevich Zastrozhin, Zhi-Jiang Zhang, Peng Zheng, Mohammad Zoladl, Jaimie D Steinmetz, Theo Vos, Mohsen Naghavi, Kanyin Liane Ong, Global, regional, and national mortality due to unintentional carbon monoxide poisoning, 2000–2021: results from the Global Burden of Disease Study 2021, The Lancet Public Health, Volume 8, Issue 11, 2023, Pages e839-e849, ISSN 2468-2667, https://doi.org/10.1016/S2468-2667(23)00185-8. (https://www.sciencedirect.com/science/article/pii/S2468266723001858) |
A Case Report of Delayed Encephalopathy After Acute Carbon Monoxide Poisoning in a Burn Patient
This case report highlights the rare but serious complication of delayed encephalopathy after acute carbon monoxide poisoning (DEACMP) in a burn patient, emphasizing diagnostic challenges, clinical progression, and the importance of monitoring for delayed neuropsychiatric sequelae.
Case Presentation:
- Patient: 48-year-old male with history of IV drug use, hepatitis C, diabetes, and deep vein thrombosis.
- Incident: Suffered 22% total body surface area burns and inhalational injury in a house fire.
- Initial Presentation: Glasgow Coma Scale of 3; carboxyhemoglobin level 8.1% (normal ≤1.5%). Treated with hydroxocobalamin and Parkland resuscitation protocol.
- Clinical Course:
- Initial neurological improvement (day 2) followed by waxing and waning neurological status, including periods of unresponsiveness, loss of reflexes, and respiratory irregularities.
- Developed hepatic failure, renal failure, and septic shock (Serratia marcescens pneumonia).
- Brain MRI (day 11): Abnormal diffusion and hyperintensity in thalami; intrinsic T1 shortening in basal ganglia—consistent with CO toxicity.
- Patient deteriorated further, lost rectal tone, required multiple vasopressors, and transitioned to comfort care before expiring on hospital day 13.
Key Clinical Insights:
- DEACMP Diagnosis:
- DEACMP is a delayed neuropsychiatric syndrome occurring days to weeks after acute CO poisoning, often following a period of apparent recovery.
- Diagnosis is supported by neuroimaging findings (e.g., basal ganglia and thalamic abnormalities) and fluctuating neurological symptoms.
- Risk Factors & Pathophysiology:
- Prolonged CO exposure, loss of consciousness, and delayed treatment are known risk factors.
- Proposed mechanisms include mitochondrial oxidative stress, neuroinflammation, apoptosis, and demyelination.
- Treatment Challenges:
- No established cure for DEACMP.
- Emerging therapies include hyperbaric oxygen (HBO), mesenchymal stem cell transplantation, and neuroprotective agents (e.g., N-butylphthalide, dexamethasone), though evidence is limited.
- Clinical Implications:
- Burn patients with inhalational injury should be closely monitored for CO poisoning and delayed neurological sequelae, even after initial stabilization.
- DEACMP should be considered in patients with unexplained neurological decline after CO exposure, especially with supportive MRI findings.
Conclusion:
This case underscores the severity and mortality risk associated with DEACMP, particularly in polytrauma patients. Increased clinical vigilance, early neuroimaging, and consideration of evolving therapies are essential in managing this complex condition. Further research is needed to establish effective treatment protocols and improve outcomes for patients with DEACMP.
Recommendations:
- Maintain high suspicion for DEACMP in burn/CO poisoning cases with delayed neurological changes.
- Incorporate advanced neuroimaging (MRI) in diagnostic workup.
- Explore multidisciplinary approaches, including potential neuroprotective and regenerative therapies, in consultation with neurology and toxicology specialists.
| REFERENCE: Patrick J. Kennedy, Allison Chowdhury, Chinaemelum Akpunonu, Ariel Rodgers, Nicole Bernal, John Loftus, A case of delayed encephalopathy after acute carbon monoxide poisoning in a burn patient, Burns Open, Volume 12, 2025, 100424, ISSN 2468-9122, https://doi.org/10.1016/j.burnso.2025.100424. (https://www.sciencedirect.com/science/article/pii/S246891222500032X) |
Exhaled Carbon Monoxide Concentration In Correlation To Clinical Parameters To Detect Carbon Monoxide Poisoning Among Fire Victims In An Egyptian Emergency Department
This Egyptian study aimed to evaluate the utility of exhaled carbon monoxide (eCO) measurement as a non-invasive, rapid diagnostic tool for detecting CO poisoning in fire victims with mild to moderate burn injuries, especially in settings where standard carboxyhemoglobin (COHb) testing is unavailable.
Study Design & Population:
- Case-control study with 40 fire victims (non-smokers, presenting within 24 hours of flame burns) and 40 matched healthy controls.
- Excluded: severe burns, lip burns, pre-existing medical conditions.
- eCO measured using CO Check Pro device upon ED arrival, before oxygen therapy.
- Clinical parameters assessed: symptoms, burn severity, duration of exposure, crowding index, and serum lactate.
Key Findings:
- Elevated eCO in Fire Victims:
- Median eCO level was significantly higher in fire victims (4.5 ppm) compared to controls (1.5 ppm) (p < 0.001).
- 37.5% of fire victims met criteria for mild CO poisoning (eCO ≥13 ppm and/or elevated lactate + symptoms).
- Correlations with Exposure & Clinical Markers:
- Positive correlations between eCO levels and:
- Serum lactate (r = 0.54, p < 0.001)
- Duration of flame exposure (r = 0.59, p < 0.001)
- Crowding index (r = 0.49, p = 0.009)
- No moderate or severe CO poisoning cases were detected based on eCO.
- Clinical & Environmental Risk Factors:
- 52.5% of victims exhibited symptoms suggestive of CO toxicity (e.g., dizziness, headache, dyspnea).
- Most fires occurred in closed spaces (77.5%), often at home or workplace.
- Overcrowding and longer exposure times were significantly associated with higher eCO levels.
- Burn Characteristics:
- Majority had mild burns (72.5%), primarily first-degree.
- 81.8% of moderate burn patients had mild CO poisoning.
Conclusion:
Exhaled CO measurement is a valuable, accessible, and non-invasive tool for early detection of CO poisoning in fire victims, particularly in resource-limited emergency departments where COHb testing may not be readily available. The strong correlation between eCO levels, clinical symptoms, and serum lactate supports its use as a reliable indicator of CO exposure.
Clinical & Public Health Implications:
- Early screening with eCO can optimize emergency triage and management of fire victims, preventing underdiagnosis of CO poisoning.
- High-risk settings (closed spaces, overcrowding, prolonged exposure) should trigger heightened suspicion and routine eCO testing.
- This approach is especially relevant for African and low-resource contexts where fire-related injuries and CO poisoning are prevalent but diagnostic resources are limited.
Recommendations:
- Integrate eCO testing into standard emergency protocols for fire victims.
- Combine eCO measurement with clinical assessment and lactate testing for comprehensive evaluation.
- Increase awareness and training on CO poisoning detection in pre-hospital and emergency care settings in resource-constrained regions.
| REFERENCE: Ahmed KhalafAllah Mohamed, Amany Atef ElKareem Abouzeid, Mohamed Galal Morsi, Amira Ismail Alamelden, Aisha Safwat Saif Eldeen, Marwa Mohammed Fouad, Exhaled carbon monoxide concentration in correlation to clinical parameters to detect carbon monoxide poisoning among fire victims in an Egyptian Emergency Department, African Journal of Emergency Medicine, Volume 15, Issue 4, 2025, 100899, ISSN 2211-419X, https://doi.org/10.1016/j.afjem.2025.100899. (https://www.sciencedirect.com/science/article/pii/S2211419X25000394) |
CONCLUSION
Reflecting on the broad global data surrounding unintentional poisonings, it is clear that our relationship with household energy requires a conscious, safety-first mindset. In environmental science, we often talk about remediation, the process of cleaning up a pollutant after it has already contaminated an ecosystem. However, when dealing with an acute toxin like carbon monoxide, waiting for remediation is a losing strategy. The only truly effective methodology is strict, uncompromising source prevention and early warning deployment.
We must demystify the science behind indoor air quality and make protective habits a natural part of our everyday lives. Installing a certified detector and testing it monthly is a minimal investment that yields a massive margin of safety.
As someone who spends free hours nurturing native plants and promoting sustainable urban ecosystems in community gardens, I view our indoor home environment as a vital micro-ecosystem that demands identical care, vigilance, and respect. By remaining proactive, maintaining our appliances, and utilizing modern detection technology, we can successfully eliminate this silent hazard and ensure our homes remain genuine sanctuaries for our loved ones.
